Welcome
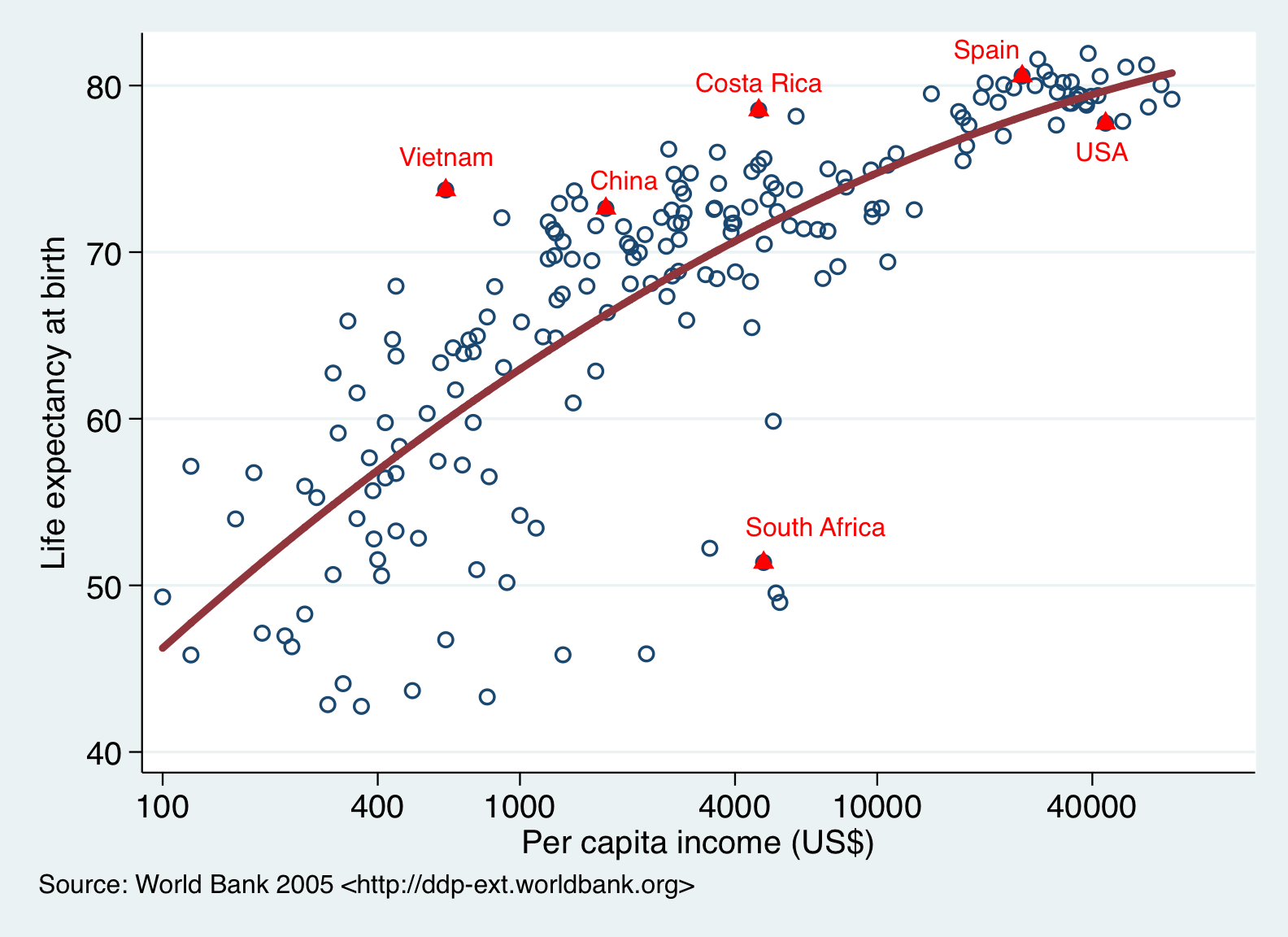
The Costa Rican Longevity and Healthy Aging Study (CRELES, or "Costa Rica Estudio de Longevidad y Envejecimiento Saludable") is a set of nationally representative longitudinal surveys of health and lifecourse experiences of older Costa Ricans. CRELES is part of the growing set of Health and Retirement Surveysbeing conducted around the world. Costa Rica is of particular interest to study given its high longevity: life expectancy is greater than that of the United States, despite being a middle income country with about one-fifth the per capita income and one-tenth the per capita health spending. CRELES is now composed of multiple waves of data from two birth cohorts.
Figure 1. Life expectancy and income in countries of the world circa 2005: Over- and under-achievers.
Family of Studies
The original CRELES Pre-1945 cohort is a nationally representative sample of nearly 3000 Costa Rican residents born in 1945 or before. Baseline CRELES household interviews were conducted primarily in 2005, with 2-year follow-up interviews in 2007 and 2009. The study was conducted by the University of Costa Rica's Centro Centroamericano de Población (CCP) in collaboration with the Instituto de Investigaciones en Salud (INISA), with the support of the Wellcome Trust (grant 072406). The Principal Investigator is Luis Rosero-Bixby, with Co-Principal Investigators Xinia Fernández (University of Costa Rica) and William H. Dow (University of California, Berkeley). Detailed description of CRELES Pre-1945.
Figure 2. Density plots of coronary heart disease biomarkers in Costa Rica (CRELES, dashed lines) and the United States (NHANES, solid lines), men and women, age 60+
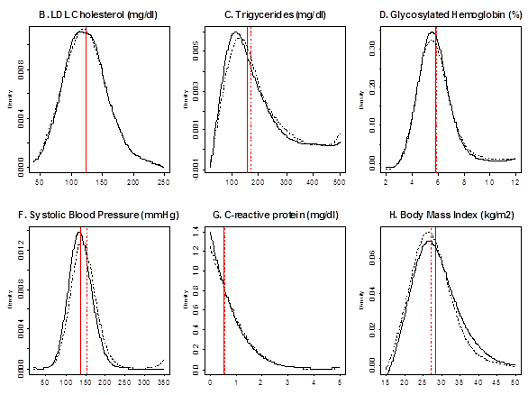
Source: Rehkopf D, Dow WH, Rosero-Bixby L; Differences in the association of cardiovascular risk factors with education: a comparison of Costa Rica (CRELES) and the United States (NHANES). J Epidemiol Community Health, 64(9):821-8, 2010.
The CRELES 1945-1955 Retirement Cohort (RC) is a sample of Costa Rican residents born 1945-1955, first interviewed starting in 2010 with a second wave starting in 2012. The sample includes about 2,800 baseline long-form interviews with targeted age-eligibles plus about 1,400 interviews with their spouses (regardless of age), conducted between January 2010 and December 2011. The CRELES-RC also includes a supplemental sample of short-form interviews conducted between January 2012 and January 2013 with about 500 initially non-responding target individuals so as to study response-rate patterns which may be especially systematic in working age populations. This study was again conducted by the University of Costa Rica’s Centro Centroamericano de Población, in collaboration with the University of California at Berkeley, with funding from the U.S. National Institute on Aging (grant R01AG031716). The Principal Investigator is William H. Dow (University of California, Berkeley) with Co-Principal Investigators Luis Rosero-Bixby and Gilbert Brenes (University of Costa Rica).
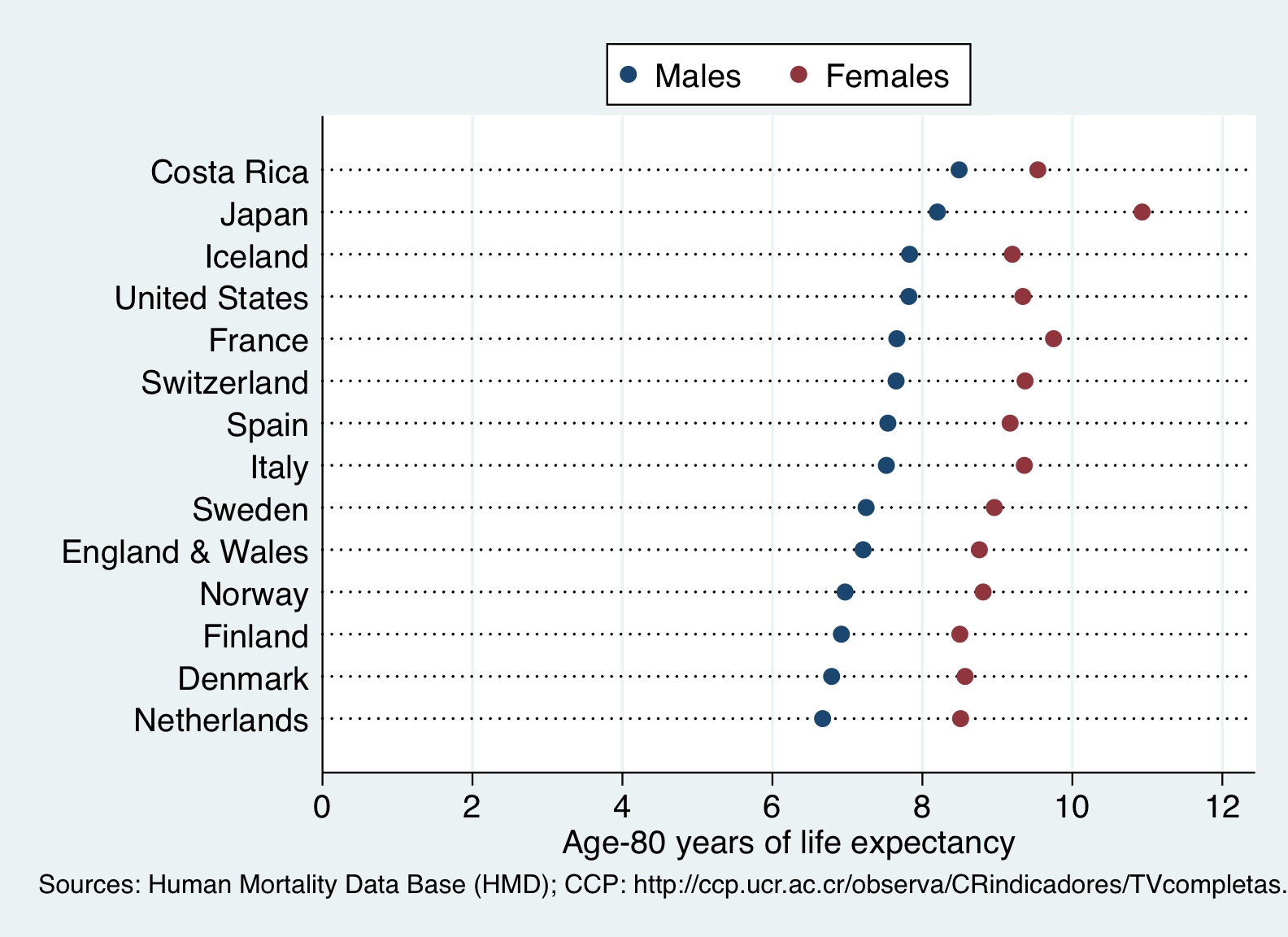
Figure 3. Age-80 life expectancy by sex for selected countries 2000-2005, ordered by male life expectancy.
CRELES data are well-suited for studying longevity determinants, relationships between socioeconomic status and health, stress and health, patterns of health behaviors, and the effects of Costa Rica’s rapid 1960s fertility decline. The CRELES surveys are distinguished by extensive measurement of health indicators as well as biomarkers. The 2005 wave of the CRELES Pre-1945 cohort included fasting blood and overnight urine collection, with blood collection repeated in 2007. The 2010 CRELES-RC drew (non-fasting) venous blood to measure cholesterol, C-reactive protein, and HbA1c. DNA has been extracted for both cohorts. Other objective health indicators include anthropometrics and observed mobility. The CRELES surveys are also distinguished by linkages with the Costa Rican National Death Index, which has allowed on-going monitoring and follow-up of mortality events, which are also studied through a surviving family interview. CRELES public use data files contain information on a broad range of topics including self-reported physical health, psychological health, living conditions, health behaviors, health care utilization, social support, work, and socioeconomic status.